The Dreaded Hamstring Injury
Recurring Hamstring Injuries and Lumbo-Pelvic Instability

Hamstring injuries are prevalent in many sporting and training environments. They are the curse of many top athletes and urban warriors alike and have a horrible tendency to recur with monotonous regularity.
In the past, rehab specialists and trainers may have fallen prey to the hypothesis that "if it keeps tearing, it must be tight and therefore needs a stretch."
In this article I would like to pose a different hypothesis. One that looks at the length-tension relationships between the hamstrings at the back of the pelvis and quads and hip flexors at the front of the pelvis. We’ll look at how this relationship can contribute to these types of injuries.
Firstly an anatomy review.
Most of us are familiar with the fact that the hamstrings arise from the ischial tuberosities (sit bones) of the pelvis and insert in to their respective points of attachment below the knee. The hamstrings therefore flex the knee and assist gluteus maximus with hip extension. When shortened and over-active posturally they will also draw the pelvis down at the back into a posterior tilt.
The quadriceps is made up of four muscles as the name suggests. The 3 vasti muscles arise from the femur and insert into the patella. Rectus femoris originates from the anterior inferior iliac spine at the front of the pelvis and also inserts into the patella. The vasti muscles extend the knee; rectus femoris also extends the knee and is a hip flexor
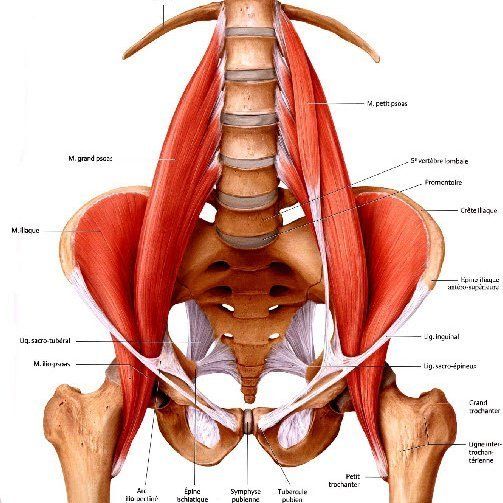
Other muscles which flex the hip include psoas and iliacus, tensor fascia lata and to a lesser degree sartorius.
The hip flexors when posturally over-active and shortened will draw the pelvis down at the front, creating an anterior tilt of the pelvis, keeping the hip in a degree of hip flexion.
Let’s get back to our recurrent hamstring injury scenario. Suppose that Jane Jogalot (an avid long distance runner) is suffering from the hamstring curse. No matter how much she stretches her hamstring, she can’t run more than 20 minutes without experiencing a tightening/straining feeling down the back of her right thigh which forces her to stop. She’s been diagnosed as having a Grade Two muscle strain of this hamstring.
The remedy - soft tissue work and progressive stretches???
But hang on - let’s look at Jane’s pelvis. Jane has a slight anterior pelvic tilt and due to her running style she is very quad-dominant. This, along with weak gluteals is allowing her pelvis to be drawn down at the front into the anterior tilt with associated shortening of ilio-psoas and tensor fascia lata.
As a sports therapist this effect can be assessed by:
A) The Wall Standing Test - Standing with the heels, buttocks and upper back in contact with the wall. The client slides their hand into the gap between the lower back and the wall. The fingers should slide behind the back to the level of the knuckles and no further. Jane might find that she can get her whole hand behind her back due to her anterior pelvic tilt and subsequent increased lumbar lordosis.
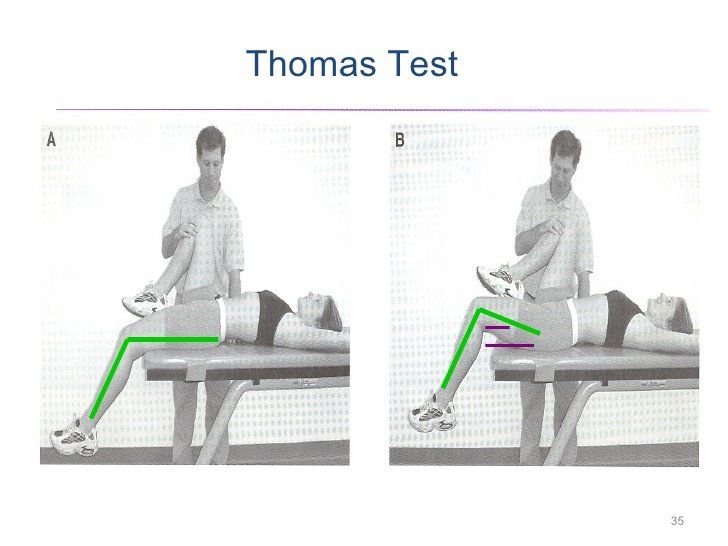
B) Hip Flexor or Thomas Test - Lying on her back on the edge of a table with her opposite knee drawn up to flatten the lower back. The hanging leg should remain in contact with the table. In Jane’s case her thigh sits up off the table with an extended knee indicating tension of her rectus femoris and possibly her hip flexors.
A hamstring test in lying reveals that Jane’s hamstrings are of normal length. Care must be taken when testing the hamstrings to allow for tight hip flexors. Occasionally the hamstrings will test "short" because the pelvis is held in an anterior tilt during the test. This restricts the straight leg raise due to pre-tensioning of the hamstring muscle fibres as they are already on a slight stretch. To compensate for this the opposite leg to the one being tested may need to be bent a little and supported on a pillow to allow the back to flatten - then re-test the hamstrings which now allows a normal range of motion to be observed (i.e.80 - 90 degrees of hip flexion with the knee in extension).
So if her hamstrings aren’t tight - why does Jane continue to have this problem??
With the anterior tilt, Jane’s hamstrings are pre-lengthened which creates extra length tension when she heel strikes. The hamstrings are unable to decelerate the limb against the pull of the hip flexors and quads at the end of the swing phase to achieve heel contact. There is a delay in the firing sequence of the hamstrings which eventually occurs with the fibres too elongated, which results in overstraining, micro-tearing and discomfort.
So if her hamstrings aren’t tight - why does Jane continue to have this problem??
With the anterior tilt, Jane’s hamstrings are pre-lengthened which creates extra length tension when she heel strikes. The hamstrings are unable to decelerate the limb against the pull of the hip flexors and quads at the end of the swing phase to achieve heel contact. There is a delay in the firing sequence of the hamstrings which eventually occurs with the fibres too elongated, which results in overstraining, micro-tearing and discomfort.
These resistance exercises might include:
Hamstring Curls - Seated, lying or standing.
Swiss Ball Hamstring Curls.
Leg Press for Gluteus Maximus.
These are just a few of the exercises that may be appropriate in Jane’s case - there are many others.
The resistance applied during these exercises will depend on Jane’s tissue tolerance at each stage of her rehab. They should be pain free.
Obviously, Jane is a fictitious character. However, this scenario is quite common in the clinical arena. Don’t always assume that "if it hurts - it needs a stretch". Correct management always boils down to a thorough assessment and specific prescription of exercises to meet the needs of the individual. If you have a reoccurring muscular problem let our sports therapist assess your muscles and prescribe a suitable workout programme.
References
(1) Kendall, McCreary,Provance, Muscles Testing and Function, Williams and Wilkins.
(2) Paul Chek Seminars - C.H.E.K.Institute: Scientific Core Conditioning Seminar
(3) Swiss Ball Training Seminar
(4) Frank Netter, Human Atlas of Anatomy - CD Rom

Richard Watson
Sports Therapist